Adults with normal renal function (GFR ≥ 90 mL/min): Reduction in the risk or delay of the onset of type 2 diabetes: Metformin should only be considered where intensive lifestyle modifications for 3 to 6 months have not resulted in adequate glycaemic control.
The therapy should be initiated with one tablet Glucophage XR 500 mg once daily with the evening meal.
After 10 to 15 days dose adjustment on the basis of blood glucose measurements is recommended (OGTT and/or FPG and/or HbA1C values to be within the normal range). A slow increase of dose may improve gastro-intestinal tolerability.
It is recommended to regularly monitor (every 3-6 months) the glycaemic status (OGTT and/or FPG and/or HbA1c value) as well as the risk factors to evaluate whether treatment needs to be continued, modified or discontinued.
A decision to re-evaluate therapy is also required if the patient subsequently implements improvements to diet and/or exercise, or if changes to the medical condition will allow increased lifestyle interventions to be possible.
500 mg: The maximum recommended dose is 4 tablets (2000 mg) once daily with the evening meal.
750 mg: The maximum recommended dose of Glucophage XR 750 mg is 2 tablets (1500 mg) once daily with the evening meal.
1,000 mg: The maximum recommended dose of Glucophage XR 1000 mg is 2 tablets (2000 mg) once daily with the evening meal.
Monotherapy or combination with other oral antidiabetic agents: 500 and 750 mg: The usual starting dose is one tablet once daily with the evening meal.
After 10 to 15 days the dose should be adjusted on the basis of blood glucose measurements. A slow increase of dose may improve gastro-intestinal tolerability.
In patients already treated with metformin tablets, the starting dose of Glucophage XR should be equivalent to the daily dose of metformin immediate release tablets.
If transfer from another oral antidiabetic agent is intended: discontinue the other agent and initiate Glucophage XR at the dose indicated previously.
500 mg: The maximum recommended dose is 4 tablets daily.
Dosage increases should be made in increments of 500mg every 10-15 days, up to a maximum of 2000mg once daily with the evening meal.
750 mg: The maximum recommended dose is 2 tablets once daily with the evening meal.
1,000 mg: Glucophage XR 1000 mg should be taken once daily with the evening meal at a maximum recommended dose of 2 tablets per day.
Glucophage XR 1000 mg is intended as a maintenance therapy for patients treated with either 1000 mg or 2000 mg of metformin hydrochloride. On switch, the daily dose of Glucophage XR should be equivalent to the daily dose of metformin hydrochloride.
In patients treated with metformin hydrochloride at a dose above 2000 mg daily, switching to Glucophage XR is not recommended.
For patients new to metformin hydrochloride, the usual starting dose of Glucophage XR is 500 mg or 750 mg once daily given with the evening meal. After 10 to 15 days the dose should be adjusted on the basis of blood glucose measurements. A slow increment in dose may improve gastrointestinal tolerability.
If glycaemic control is not achieved on 2000 mg metformin hydrochloride extended release once daily, patients may be switched to standard metformin hydrochloride immediate-release to a maximum dose of 3000 mg daily.
In the event of transfer from another oral antidiabetic agent, titration should begin with Glucophage XR 500 mg before switching to Glucophage XR 1000 mg as indicated previously.
Combination with insulin: Metformin and insulin may be used in combination therapy to achieve better blood glucose control.
500 mg and 1,000 mg: The usual starting dose of Glucophage XR is one tablet once daily with the evening meal, while insulin dosage is adjusted on the basis of blood glucose measurements.
750 mg: The usual starting dose of Glucophage XR is one tablet once daily up to a maximum of 1500 mg with the evening meal, while insulin dosage is adjusted on the basis of blood glucose measurements.
1,000 mg: After titration, switch to Glucophage XR 1000 mg should be considered.
Elderly: Due to the potential for decreased renal function in elderly subjects, the metformin dosage should be adjusted based on renal function. Regular assessment of renal function is necessary (see Precautions).
Benefit in the reduction of risk or delay of the onset of type 2 diabetes mellitus has not been established in patients 75 years and older (see Pharmacology: Pharmacodynamics under Actions) and metformin initiation is therefore not recommended in these patients (see Precautions).
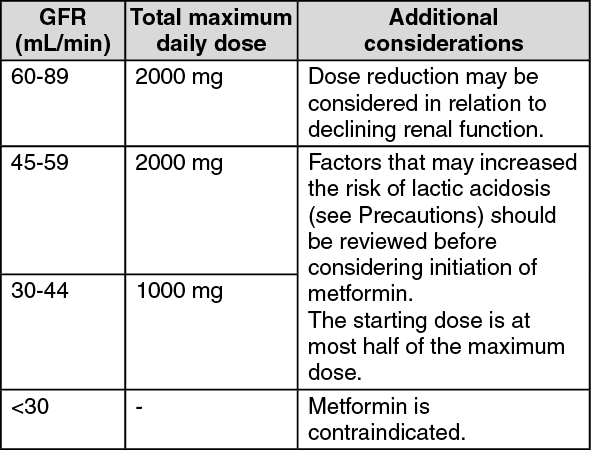
Renal impairment: A GFR should be assessed before initiation of treatment with metformin containing products and at least annually thereafter. In patients at an increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months. (See table.)
 Click on icon to see table/diagram/image
Paediatric Population:
Click on icon to see table/diagram/image
Paediatric Population: In the absence of available data, Glucophage XR should not be used in children.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
